
Written by Lee Jarvis. Proofreading and editing by Rosemary Bonnell.
I feel fortunate to write for the CJO as doing so has given me the opportunity to interview many other Osteopathic Manual Therapists. These interviewees are individuals with years of experience and significant teaching backgrounds in numerous subjects. During these interviews it unsurprisingly (and quickly) turns into manual demonstrations that are quite unique to that practitioner, created by them through their process of experimentation over time. Some of these demonstrations are clever and practical, some are easy on the body of the practitioner, and some feel just wonderful for the patient. The demonstration by Kristen Jarvis illustrated in this article was all of those things together and thus more than worthy of a complete write-up.
In the latter part of our interview (parts 1, 2, and 3 having already been written and posted), Kristen was demonstrating some manual methods to different areas of the body with myself as the patient and eventually worked her way up to the neck. As she is an experienced practitioner there was no hesitation and Kristen grasped my head and neck in a hold I had not seen before. This seems to be so often the case with experienced practitioners, what they consider a normal tool of daily use would be entirely unthought of by another practitioner.
Standing at the side of the top of the table Kristen faced the patient (who was me, the author, an only marginally relevant character in this story).

Kristen’s up-table hand (the left in this demonstration) wrapped from the posterior side of the cranium to the Atlanto-Occipital region. The palm was holding the Occiput region and the fingers had a slight bend allowing the fingertips to rest on the Suboccipital area. Kristen’s down-table hand (the right in this demonstration) reached cross-table and grasped the upper cervical segments, perpendicular to the vertical Cervical spine. The right hand wrapped from anterior to posterior ending with the palm lightly holding the bulk of the left side neck musculature and the bent fingers palpating the cervical vertebrae.

When Kristen had the neck and head secured in this hold, she stood up just a little straighter from her leaned over position. This standing up straighter easily lifted the head and neck off the table. I feel it worth mentioning that it was a very comfortable position to experience as the patient, which is not everything in OMT but certainly well worth doing when possible. When done well the patient feels as if their neck is “floating” and this is a product of both the security of the hold as well as the smooth movements of the practitioner.

When Kristen leaned backward and lifted up just a little with her down-table hand this created extension in the cervical spine.

Initially, the hand holding the occiput (up-table hand) stayed relatively still
during this demonstration of the movement, however, Kristen showed that she could also drop the up-table hand/occiput downward to create more significant cervical extension.
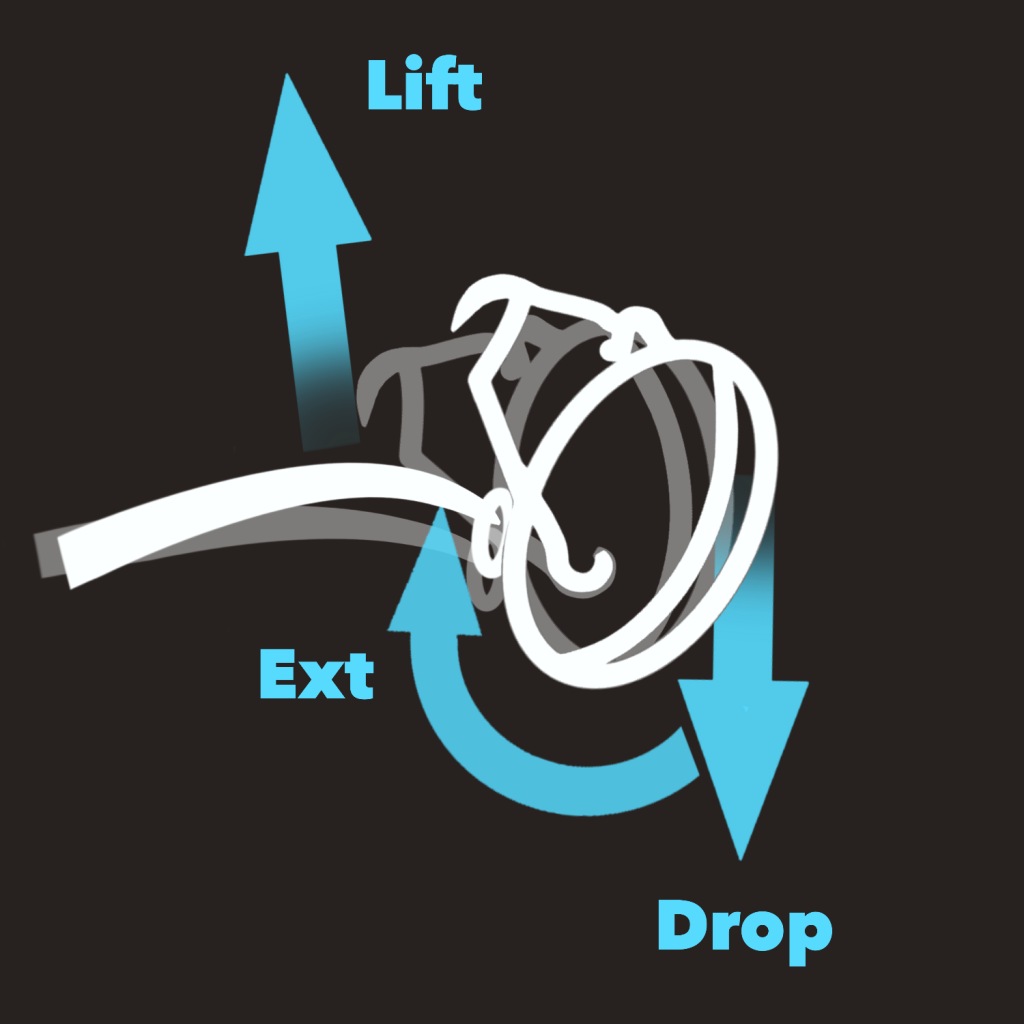
Where the hand on the cervical spine is positioned, whether still or moving, will define where the extension is concentrated (this being traditionally called a “fixed point”).
Due to the hold, the weight of the head, and the nature of gravity it should be no surprise that this maneuver is particularly useful for cervical areas that favour flexion, though it is not limited to that exclusively.
Kristen then demonstrated that the up-table hand can move up and down to create Atlanto-Occipital flexion and extension. This movement can be easily done with no practitioner muscular effort by simply leaning to the left or right.
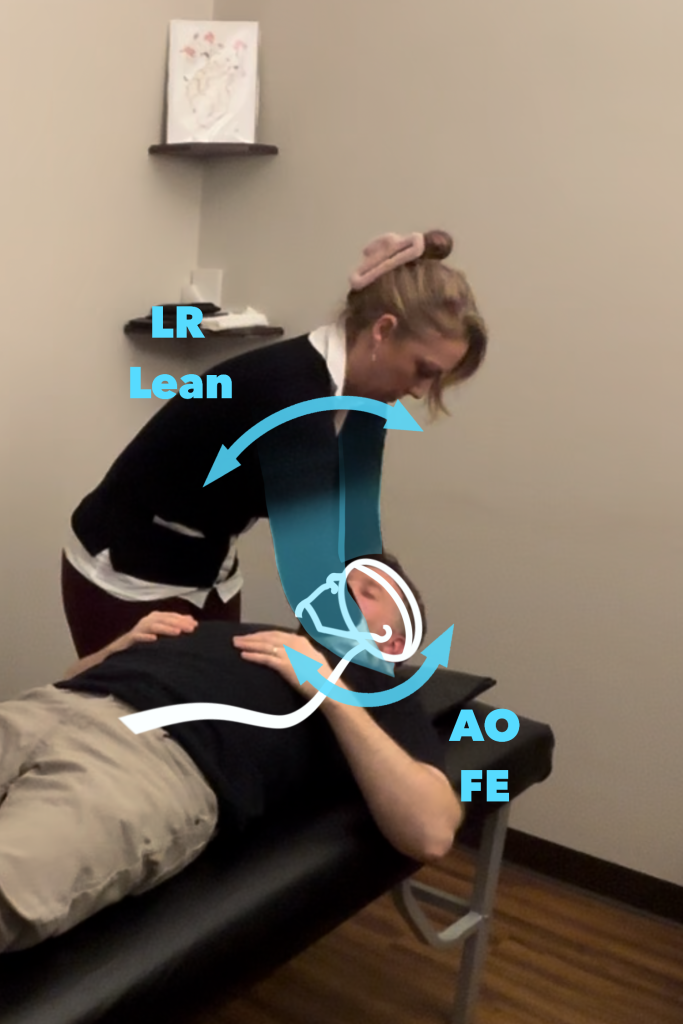


Then it was demonstrated that by moving the up-table hand away or towards the practitioner (to the patients left or right) that the hold can create side-bending as needed.
Lastly, the up-table hand fingers are available to press into the Suboccipital muscles as a form of gentle inhibition as needed.
As always the patient in front of us determines the specifics of how any hold or maneuver should be applied and utilized in treatment. I was so impressed and happy to have been shown this method that I immediately started using it in my own practice.
I would like to thank Kristen for demonstrating this to me as well as taking time out of her busy schedule for an interview. She has shown that she cares greatly about her practice and patients.